Abstracts
Diffuse plane normolipemic xanthoma is a rare disease, of a group of clinical syndromes called histiocytoses, characterized by the presence of yellowish or yellow-orange plaques, distributed symmetrically on the cutaneous surface and usually accompanied by xanthelasma. It affects mainly adults and it may cause discrete changes in serum lipids. The case of an 85-year-old female patient who has been showing extensive asymptomatic yellow-orange plaques in the trunk and abdomen for a year is reported. Laboratory tests did not show an increase in serum lipids or the occurrence of reticuloendothelial disorders.
Multiple myeloma; Paraproteinemias; Xanthomatosis
O xantoma plano difuso normolipêmico é doença rara, do grupo das histiocitoses, caracterizada pelo aparecimento de placas amareladas ou amarelo-alaranjadas, distribuídas simetricamente na pele e geralmente acompanhadas por xantelasma. Acomete principalmente adultos, podendo ou não apresentar alterações discretas dos lípides séricos. Relata-se o caso de uma paciente do sexo feminino, de 85 anos, há um ano com extensas placas amarelo-alaranjadas no tronco e abdome, assintomáticas. Os exames laboratoriais não demonstraram aumento dos lípides séricos, nem ocorrência de desordens retículo-endoteliais.
Mieloma múltiplo; Paraproteinemias; Xantomatose
DERMATOPATHOLOGY
ISixth-year graduate student of Medicine at Faculdade de Medicina (FAMED) - Universidade Federal de Mato Grosso do Sul (UFMS) - Campo Grande (MS), Brazil
IIPh.D. in Dermatology at Universidade São Paulo (USP), and Professor at Universidade Federal de Mato Grosso do Sul (UFMS) - Campo Grande (MS), Brazil
IIIResident physician in Dermatology at Faculdade de Medicina (FAMED) - Universidade Federal de Mato Grosso do Sul (UFMS) - Campo Grande (MS), Brazil
IVPh.D. student in Oncology at Universidade de Sao Paulo (USP), M.S. in Health Sciences at Universidade de Brasilia (UNB), Professor of Special Pathological Anatomy at Faculdade de Medicina (FAMED) - Universidade Federal de Mato Grosso do Sul (UFMS), Campo Grande (MS), Brazil
VThird-year graduate student of Medicine at Faculdade de Medicina (FAMED) - Universidade Federal de Mato Grosso do Sul (UFMS) - Campo Grande (MS), Brazil
Mailing Address
ABSTRACT
Diffuse plane normolipemic xanthoma is a rare disease, of a group of clinical syndromes called histiocytoses, characterized by the presence of yellowish or yellow-orange plaques, distributed symmetrically on the cutaneous surface and usually accompanied by xanthelasma. It affects mainly adults and it may cause discrete changes in serum lipids. The case of an 85-year-old female patient who has been showing extensive asymptomatic yellow-orange plaques in the trunk and abdomen for a year is reported. Laboratory tests did not show an increase in serum lipids or the occurrence of reticuloendothelial disorders.
Keywords: Multiple myeloma; Paraproteinemias; Xanthomatosis
INTRODUCTION
Xanthomas are cutaneous lesions of variable morphology caused by localized deposits of lipids in the skin. These deposits occur inside histiocytes, which acquire a foamy aspect. Xanthomas are the externalization, in the skin, of diseases resulting from local or general disturbances in lipid metabolism.1 In approximately half of the cases, they occur in the absence of hyperlipidemia and hypercholesterolemia.2
The term 'plane xanthoma' morphologically describes a group of xanthomatous lesions, which appear in the form of plane or slightly elevated maculae.3
Different classifications of plane xanthomas have been presented. Generally, they can be divided into two groups: 1) plane xanthomas with increased serum levels of lipids, and 2) plane xanthomas with normal serum levels of lipids. The second group can be, in its turn, subdivided into three types: 1) idiopathic; II) associated with multiple myeloma, monoclonal gammopathies, and, less frequently, with lymphoproliferative disorders, and III) associated with abnormalities in the structure and content of lipoproteins.4
Diffuse plane xanthoma (DPX) is a cutaneous disorder used to refer to more widespread and diffuse skin lesions, which are usually associated with type II in the classification of plane xanthomas.4
Moreover, diffuse plane xanthomas are part of hystiocytic syndromes, which constitute a group of disorders with clinical features varying from localized and benign to those widespread and with negative prognosis. Since 1987, they have been grouped into three categories: Langerhans cell histiocytosis (LCH) or class I; mononuclear phagocytic histiocytosis (non-Langerhans) or class II, and malignant histiocytosis or class III.5 Diffuse plane xanthoma belongs to class III, based on its immunohistochemical characteristics, which classify histiocytosis. 6
CASE REPORT
Female patient, 85 years old, white, native of Campo Grande, MS, Brazil. A year ago she noticed the appearance of asymptomatic yellowish skin lesions in her thorax and abdomen.
Dermatologic examination revealed plane yellow-orange plaques with irregular, well-defined borders (Figure 1), of variable dimensions, symmetrically distributed in the cutaneous surface, in the anterior thorax and abdomen (Figure 2), dorsum (Figure 3) and buttocks. Face, cervical region, mucous membranes, limbs, and palmoplantar regions were free of lesions.
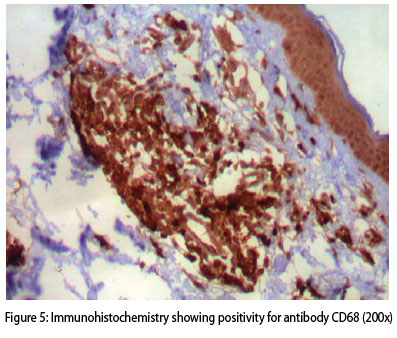
The anatomopathological exam, stained with hematoxylin-eosin, showed epidermis with spongiotic foci, lymphomononuclear cell exocytosis, and papillary dermis evidentiating focal points of lymphomononuclear infiltrate permeated by aggregates of xanthomatous cells (Figure 4) and absence of malignant signs. Immunohistochemical stains showed positivity for antibody CD68 (Figure 5) and negativity for marker CD1a and protein S100.
The complementary examinations: glycemia, sodium, potassium, hepatic and renal functions, LDH, ferritin, total and fraction proteins, alkaline phosphatase, gamma-GT, total and fraction bilirubin, erythrocyte sedimentation rate (ESR), mucoproteins, thyroid hormones, eletroctrophoresis of serum and urine protein, immunoglobulin IgM, FAN test, P-Anca and C-Anca, rheumatoid factor, anti-cardiolipin IgG, anti-cardiolipin IgM, CH50, C3, C4, lipid profile (total cholesterol 130 mg/dl, LDL 85.3 mg/dl, HDL 28.1 mg/dl, triglycerides 83 mg/dl), and electrophoresis of lipoproteins (alpha-lipoproteins, pre-beta-lipoproteins, beta-lipoproteins, kilomicrons) yielded normal results. Bence-Jones proteinuria and cryoglobulin were not found.
Serologic exams for hepatitis B, C, and Leishmaniasis were negative. Thoracic, cranial, and pelvic radiography showed no alterations. Bone marrow aspiration revealed absence of parasites and of infiltration by neoplastic cells.
Hemogram test results showed pancytopenia: erythrocytes, 3.63 million/mm3; leucocytes, 2640/mm3, platelet count, 93.000/mm3. Abdominal ultrasonography indicated discrete splenomegaly.
DISCUSSION
Diffuse plane normolipemic xanthoma is a well-defined clinical-pathological entity7 that affects mainly adults, of both genders, and is characterized by the development of maculae and plane or slightly elevated plaques of yellowish, yellow-orange7 or yellow-brown8 color. They vary in dimension and can be clearly demarcated or have borders with little definition. They usually have a symmetrical distribution in the body surface area. 3
Lesions occur primarily in the upper trunk, in the lateral cervical region, and limbs.3 However, any area of the body7,8, such as flexures7, abdomen9, and buttocks10, can present lesions, which are often accompanied or preceded by xanthelasma.3
Diffuse plane normolipemic xanthoma was described for the first time in 1962, by Altman and Winkelmann11, who initially believed that these cutaneous lesions were not associated with internal disturbances. Nonetheless, four years later, Lynch and Winkelmann3 confirmed that lesions were associated with reticuloendothelial system disorders, particularly multiple myeloma. Other reports showed an association of the disease with monoclonal gammopathies4,7,9 and limphoproliferative disorders.2,3,10
In a histopathological analysis, foam cells - lipid-laden macrophages - and a variable number of Touton giant cells, lymphocytes, and foamy histiocytes were seen in the outer dermis and, occasionally, they may have perivascular localization.10,12 Furthermore, focal necrobiosis has been observed in diffuse plane xanthoma (DPX) and evolution of this condition to necrobiotic xanthogranuloma has been reported. This suggests that both may represent clinical conditions of the same spectrum of diseases.10
In the case being reported, the distribution of lesions did not correspond to the typical pattern found, since they affected the anterior trunk, abdomen, dorsum, and buttocks, with absence of xanthelasma. Contrary to expectations, association of DPX with systemic alterations, especially myeloproliferative disorders, has not been observed. Isolated hypersplenism was diagnosed, which explains the occurrence of pancytopenia. Due to the frequent incidence of visceral leishmaniasis, it was important to dismiss this diagnosis.
Histopathological examination suggested the diagnosis of diffuse plane xanthoma. Since the patient did not show necrobiosis or the occurrence of granulomatous infiltration in the dermis and subcutaneous tissue13, the diagnosis of necrobiotic xanthogranuloma was dismissed in the absence of clinical symptoms. The immunohistochemistry confirmed histiocytosis of mononuclear phagocytes. 6
The pathogenesis of DPX is not clearly defined. Regarding associations with gammopathies, some authors believe that paraproteinemia-lipoproteinemia complexes are deposited in the skin.14 Others suggest the infiltration of leukemic cells in the skin with consequent xanthomization.15 Still, others consider DPX a form of non-Langerhans histiocytosis.6
One hypothesis to explain the occurrence of xanthoma in normolipemic patients is that the development of histiocyte-monocyte complexes, functionally abnormal, stimulates hyperplasia and secondary xanthomization2, which indicates the probable pathogenesis of the present case.
According to some authors, only a few cases are considered idiopathic. However, the frequency of reports with associated disease may be explained by the tendency of authors to describe them and neglect idiopathic cases.10
Since the patient did not show any criterion for diagnosis of multiple myeloma, and complementary examinations did not reveal monoclonal gammopathies or lymphoproliferative disorders, the present case is classified as diffuse plane idiopathic normolipemic xanthoma.
Because xanthomas may appear years before the occurrence of systemic disorders or hematologic disturbances, patients who have received this diagnosis need clinical long-term follow-up.

REFERENCES
- 1. Sampaio SAP, Rivitti EA. Dermatologia. 3 ed. São Paulo: Artes Médicas; 2007. p.910-9.
- 2. Maxit MJ, Paz RA. Xantoma plano difuso com artritis, serosits, eritema nodoso, vasculitis y leucemia mielomonocitica. Medicina (B Aires). 2001;61:187-90.
- 3. Lynch PJ, Winkelmann RK. Generalized plane xanthoma and systemic disease. Arch Dermatol. 1966;93:639-46.
- 4. Daoud MS, Lust JA, Kyle RA, Pittelkow MR. Monoclonal gammopathies and associated skin disorders. J Am Acad Dermatol. 1999;40:507-35.
- 5. Quattrino AL, Silveira JCG, Diniz C, Briggs MC, Vilar E. Histiocitose de células de Langerhans: relato de caso e revisão da literatura. An Bras Dermatol. 2007;82:337-41.
- 6. Luz FB, Gaspar AP, Gaspar NK, Silva MR. Os histiócitos e as histiocitoses não Langerhans em dermatologia. An Bras Dermatol. 2003;78:99-118.
- 7. Buezo GF, Porras JI, Fraga J, Sanchez E, Aragües M, Daudén E. Coexistence of diffuse plane normolipaemic xanthoma and amyloidosis in a patient with monoclonal gammopathy. Br J Dermatol. 1996;135:460-2.
- 8. Akhyani M, Daneshpazhooh M, Seirafi H, Naraghi ZS. Diffuse plane xanthoma in an otherwise healthy woman. Clin Exp Dermatol. 2001;26:405-7.
- 9. Ginarte M, Peteiro C, Toribio J. Generalized plane xanthoma and idiopathic Bence-Jones proteinuria. Clin Exp Dermatol. 1997;22:192-4.
- 10. Marcoval J, Moreno A, Bordas X, Gallardo F, Peyrí J. Diffuse plane xanthoma: Clinicopathologic study of 8 cases. J Am Acad Dermatol. 1998;39:439-42.
- 11. Altman J, Winkelmann RK. Diffuse normolipemic plane xanthoma. Generalized xanthelasma. Arch Dermatol. 1962;85:633-40.
- 12. Bragg J. Diffuse plane xanthomata. Dermatol Online J. 2005;11:4.
- 13. Macedo DM, Hirata SH, Michalany NS, Enokihara MMSS, Enokihara MY. Xantogranuloma necrobiótico solitário sem paraproteinemia. An Bras Dermatol. 2008;83:243-6.
- 14. Taylor JS, Lewis LA, Battle JD, Butkus A, Robertson AL, Deodhar S, et al. Plane xanthoma and multiple myeloma with lipoprotein-paraprotein complexing. Arch Dermatol. 1978;114:425-31.
- 15. Vail JT Jr, Adler KR, Rothenberg J. Cutaneous xanthomas associated with chronic myelomonocytic leukemia. Arch Dermatol. 1985;121:1318-20.
Diffuse plane idiopathic normolipemic xanthoma with hiperesplenism
Publication Dates
-
Publication in this collection
06 May 2010 -
Date of issue
Feb 2010